Simmaron's Science Behind the Rapamycin Trial Our new placebo-controlled rapamycin trial is based on 4 peer-reviewed publications of our work on the mechanisms and biomarkers disrupting autophagy in a subset of ME/CFS & Long-Covid patients with PEM. When our science team published that a patient subset has inactive ATG13 in 2022 (Molecular and Cellular Neuroscience study here), we went on to show how inactive ATG13 is related to mTOR activation, that inactive ATG13 can cause a version of PEM, and how we can reverse it with rapamycin, an mTOR inhibitor. We: - Demonstrated what missing ATG13 looked like in animal models, developing the first mouse models to display post-exertional malaise (PEM) - and publishing our model. (2025 Immunologic Research study here)
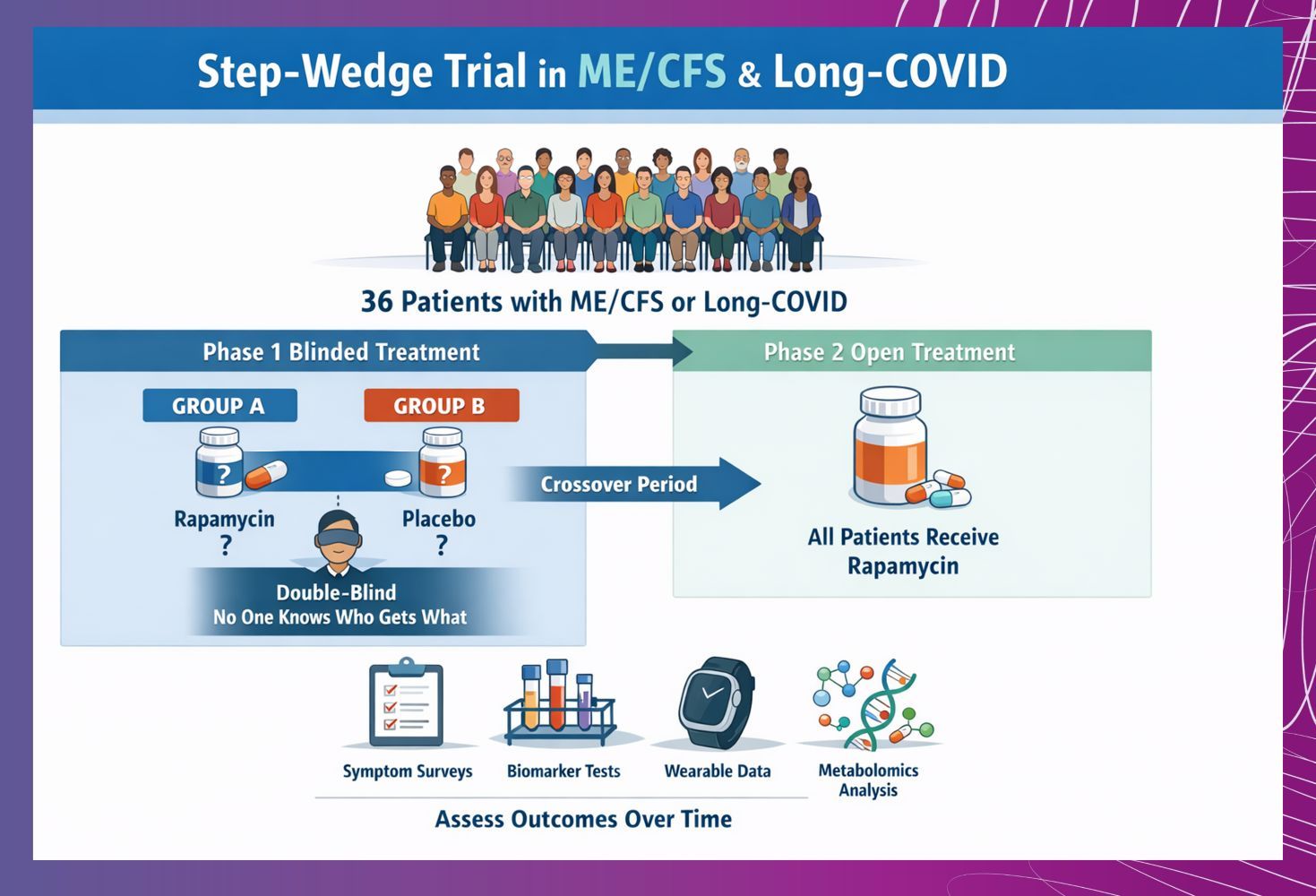
- Ran a treatment trial of mTOR inhibitor rapamycin to address dysfunctional autophagy caused by inactive ATG13, publishing Phase 1 results in high impact Journal of Translational Medicine and are now preparing a placebo-controlled trial. (2025 study here)
- Explained how missing ATG13 in cells causes symptoms of PEM, now describing in publication a cascade of inflammation that implicates new molecules and processes, to drive treatment discovery in the field. (2026 Inflammation Research study here)
- Are developing a blood test that can help predict which patients are likely to respond to rapamycin to take the guess-work out of treating ME/CFS.
|
|