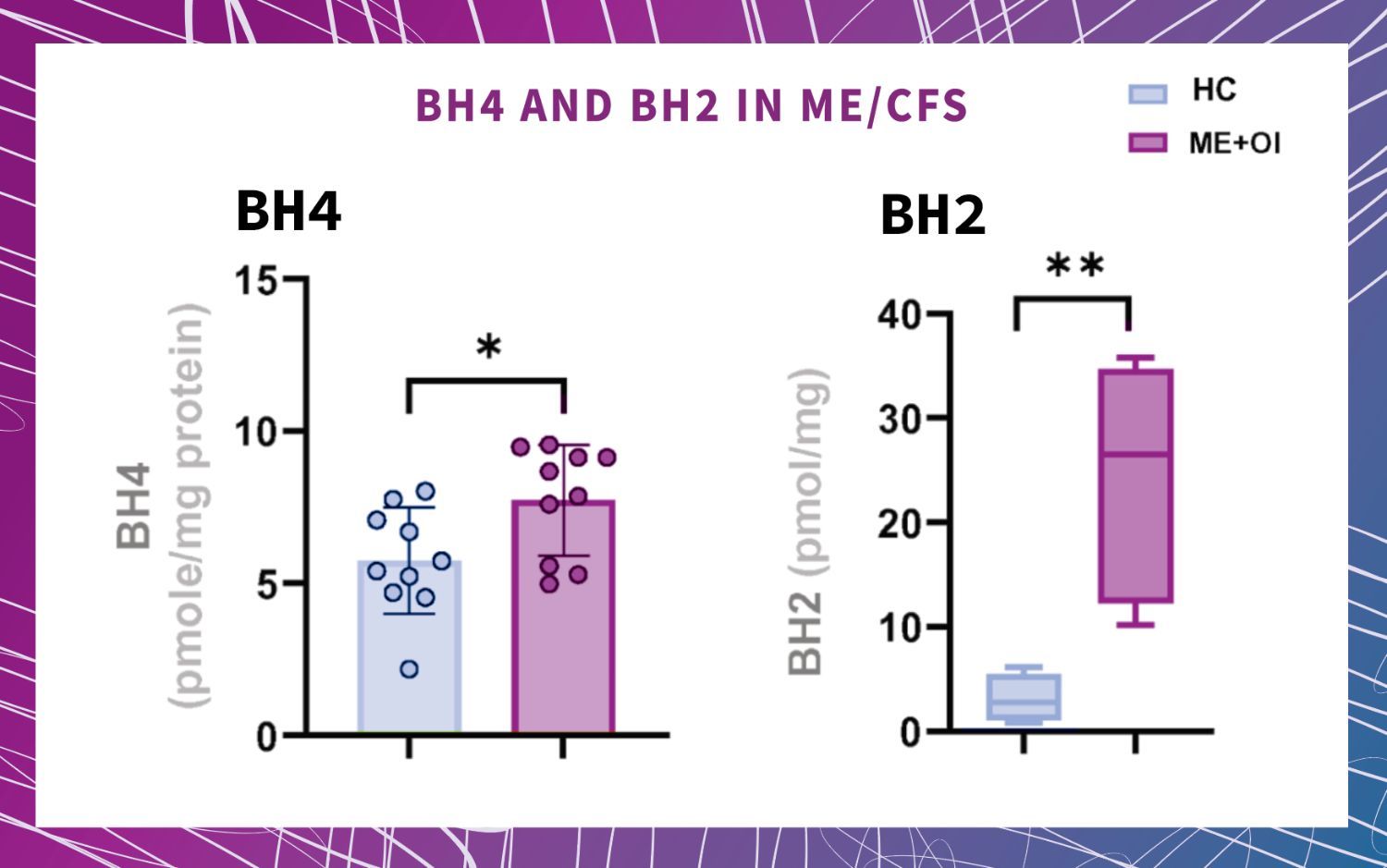
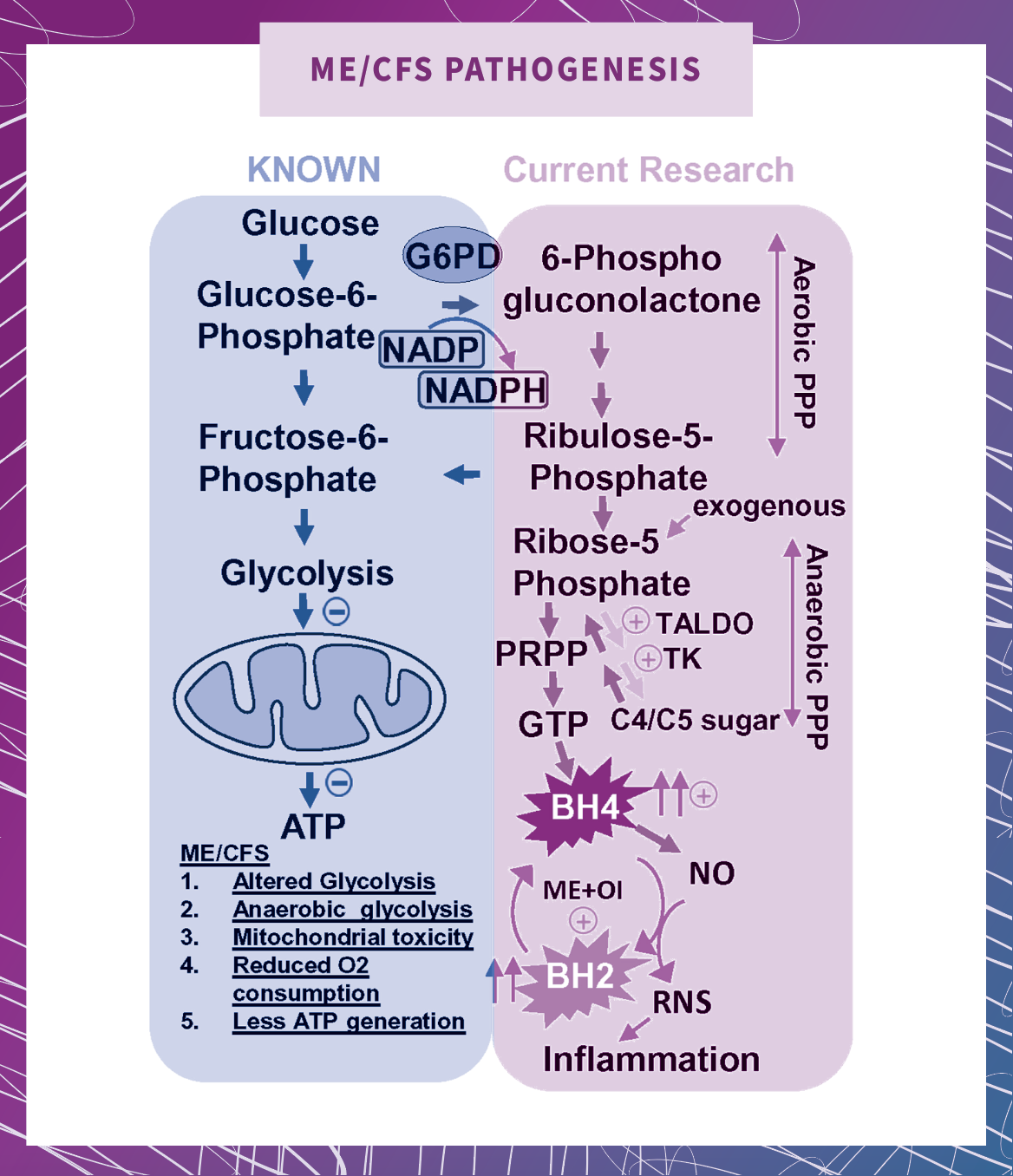
2. Elevated biopterins (BH4, BH2) contribute to inflammation in microglial cells, producing nitric oxide, which in turn lowers blood pressure through vasodilation. Nitric oxide (NO) is a culprit in orthostatic intolerance, a condition where patients feel dizzy or faint when standing or sitting up. BH4 is known to be a co-factor enzyme for production of NO, meaning it is necessary for NO. In ME+OI patients, high levels of BH4 also correlated with high levels of NO. Nitric oxide widens blood vessels, which leads to lower blood pressure and less constriction of vessels upon standing. So, understanding the cause of elevated BH4 in ME+OI patients could lead to methods for regulating orthostatic intolerance. |
|